
... And This Time, It May Lead to New Treatments
A new Science Advances paper suggests that stress-linked nerve signaling may help shape the immune attack in vitiligo. That does not mean vitiligo is “just stress.” It means the nervous system may be one more lever drug developers can try to pull.
In Brief
A new study adds detail to an old suspicion: the sympathetic nervous system may help worsen vitiligo by making the skin more attractive to autoreactive immune cells. The paper links norepinephrine-driven signaling to the production of inflammatory messengers such as CXCL9, CXCL10, IL-6, and IL-15 in skin cells. That matters because these molecules are already tied to vitiligo activity and relapse.
The practical takeaway is simple. This pathway may eventually support new treatment ideas, especially topical or combination therapies aimed at reducing neuroimmune signaling in the skin. A realistic timeline for early repurposing work is around 1 to 3 years, with small proof-of-concept human studies perhaps in 2 to 4 years, and any purpose-built therapy more likely in the 5 to 10 year range.
For years, people with vitiligo have said the same thing in one form or another: stress matters. Doctors heard it. Patients felt it. Researchers suspected it. But suspicion is not the same as mechanism.
A new paper in Science Advances adds something the field has badly needed: a more detailed biological route connecting sympathetic nerve activity to immune damage in vitiligo. In plain English, the study suggests that “fight-or-flight” nerve signals may help make the skin more welcoming to the immune attack that destroys melanocytes.
That does not mean vitiligo is “all in the nerves.” Let’s not drift into nonsense. Vitiligo is still an autoimmune disease. But this work suggests the nervous system may be acting like an accomplice — not the whole crime syndicate, but maybe the guy holding the side door open.
Definitions
- Sympathetic nervous system: the branch of the nervous system involved in the body’s stress or “fight-or-flight” response.
- Norepinephrine: a signaling molecule released by sympathetic nerves.
- CXCL9 / CXCL10: inflammatory chemokines that help attract immune cells to the skin.
- IL-15: an immune signaling molecule linked to the persistence of tissue-resident memory T cells, which may help vitiligo recur in the same places.
- Adrenergic receptors: receptors on cells that respond to norepinephrine and related stress signals.
The basic discovery
The researchers focused on the sympathetic nervous system, the branch involved in stress responses and norepinephrine release. They found evidence that abnormal sympathetic activation may contribute to the inflammatory skin environment seen in vitiligo.
More specifically, the study traced a pathway in which norepinephrine appears to act through adrenergic receptors on skin cells such as fibroblasts and keratinocytes. Those cells then produce inflammatory signals including CXCL9, CXCL10, IL-6, and IL-15. In turn, these molecules may help recruit and activate autoreactive CD8 T cells — the same immune cells already known to play a central role in melanocyte destruction.
That is what makes this paper interesting. It does not replace the existing immune model of vitiligo. It plugs the nervous system into it.
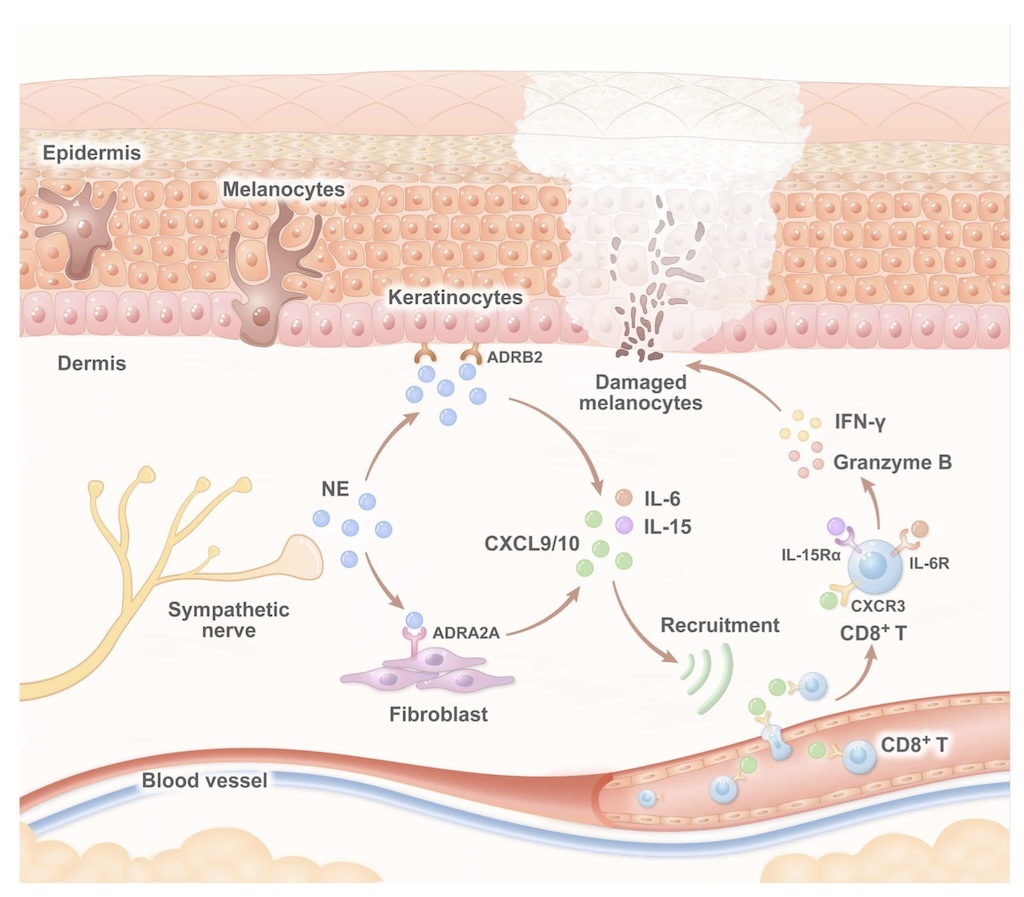
Schematic diagram of sympathetic nerves in vitiligo
Why this matters
The real value here is not the old observation that stress can worsen vitiligo. People have been saying that for ages. The real value is that this paper gives the field a more specific neuroimmune route to investigate.
Once a pathway is mapped, the conversation changes. We move from vague advice about “managing stress” to more practical questions. Can this signal be blocked locally in the skin? Can the inflammatory response be dampened before immune cells pile in? Can this be combined with existing therapies such as phototherapy or JAK inhibition?
In other words, the study gives drug developers something they like very much: actual handles.
What therapies could grow out of this?
The most obvious possibility is some form of adrenergic receptor blockade. If norepinephrine-driven signaling helps shape a hostile skin environment, then blocking that signal may reduce the cascade that attracts and sustains autoreactive immune cells.
Now for the usual reality check: a mechanistic paper is not a treatment. Nobody should be raiding the cardiology shelf and trying random beta-blockers on their skin. That is not how this works, and it is a very efficient way to create trouble where none was scheduled.
Still, the study points toward several practical directions.
1. Topical neuroimmune modulators
This is probably the most attractive idea. Vitiligo is a skin disease, and local therapy is usually easier to justify than long-term systemic treatment when safety is uncertain. A topical agent that dampens norepinephrine-linked inflammatory signaling in lesional or high-risk skin would be far more appealing than broad systemic sympathetic blockade.
2. Combination therapy
This may be where the field is really heading. One treatment could reduce the immune attack. Another could support repigmentation. A third could help calm the skin’s tendency to call autoreactive T cells back into the area. No single silver bullet, just a smarter stack.
3. Biomarker development
If this pathway proves measurable in a clinically useful way, it may help identify patients with more stress-reactive or inflammatory disease patterns. That is not glamorous, but it could be useful for trial design and treatment stratification.
What are the limits of this paper?
This is the part where the grown-ups walk in and lower the music.
The findings are promising, but they do not settle the field. Neuroimmune biology is messy, and not every study has pointed in exactly the same direction. There have already been conflicting interpretations about how central sympathetic nerves really are in driving vitiligo progression.
So this paper should be seen as an important mechanistic lead, not the final verdict. It gives the field a strong hypothesis and a possible therapeutic angle. It does not yet prove that blocking this pathway will produce meaningful clinical benefit in people.
What this page does not support
- This study does not prove that vitiligo is caused by stress alone.
- This study does not mean people should self-treat with cardiovascular drugs or over-the-counter “anti-stress” products.
- This study does not mean a new therapy is around the corner next month.
What it does support is a more serious look at the neuroimmune side of vitiligo biology — and that is useful.
Approximate timeline: when could this become a real therapy?
Drug development is not famous for its speed, charm, or respect for calendars. Still, a rough timeline is possible.
Estimated development path
| Stage | Approximate timeline | What it may involve |
|---|---|---|
| Preclinical follow-up | 1–3 years | Testing existing adrenergic modulators, clarifying receptor subtypes, refining animal and cell models, exploring topical delivery |
| Early proof-of-concept human studies | 2–4 years | Small investigator-led trials, likely in combination with phototherapy or existing immune-directed treatments |
| Purpose-built topical or combination therapy | 5–8 years | More serious dermatology-focused development if the biology holds up and funding appears |
| Approved therapy designed around this pathway | 7–10+ years | Full clinical development, larger trials, regulatory review, and commercial formulation work |
These are rough estimates, not promises. A repurposed compound could move faster. A dead-end mechanism could move nowhere at all. Science can be elegant, but drug development often behaves like airport luggage handling.
Where this could fit into the future of vitiligo treatment
The larger point is that vitiligo treatment is becoming more layered. The field already includes oxidative stress, innate immunity, adaptive immunity, tissue-resident memory T cells, and repigmentation biology. This paper adds a stronger neuroimmune angle to that map.
That is good news. Precision creates options. Options create therapies. And therapies, eventually, create better lives.
For now, the smartest conclusion is this: the sympathetic nervous system may not be the main villain in vitiligo, but it may be helping the villains get through the door. If future studies confirm that, blocking this pathway could become one more useful piece in the next generation of treatment.
Bottom line
This discovery is best viewed as an early-stage therapy lead, not an imminent cure. The shortest plausible path is repurposing work and topical experimentation over the next few years. The longer path is the design of dedicated neuroimmune treatments for vitiligo over the next decade.
That may sound slow. It is slow. But it is still progress. Once a disease leaves footprints in a pathway, drug developers start following the trail.

by Yan Valle
Prof. h.c., CEO VR Foundation
Suggested Reading
- The Immunology Of Vitiligo For Clinicians
- The Immunology Of Vitiligo In Plain English
- Rethinking Vitiligo – Five Distinct Faces of a Complex Disease
- Sixty Years of Vitiligo Research: Where We’ve Been and Where We’re Going
- Ayahuasca as a Potential Therapy for Vitiligo. A Journey into the Mind-Body Connection
Listen to Deep Dive in Vitiligo Podcast
- Topical Rapamycin — Vitiligo’s Next Big Hope? (Ep. 54)
- Nanotechnology for Vitiligo — Tiny Tools, Big Hopes (Ep. 49)
- Sixty Years Of Vitiligo Research — Where Are We Now and What Comes Next? (Ep. 35)
- Behavioral Epigenetics: How Stress Affects Vitiligo (Ep. 22)
- Mind, Body, and Ayahuasca: An Uncharted Approach to Vitiligo (Ep. 16)
References
-
Sympathetic nerve aggravates autoimmune skin disease via NE–adrenergic receptor axis: Neuroimmune cross-talk insights from vitiligo (Online or PDF)
Medical note: This article is for educational purposes and should not be treated as personal medical advice. Any treatment decisions should be discussed with a qualified healthcare professional.